Interesting Case done at Indo US Superspeciality Hospital, Ameerpet, Hyderabad
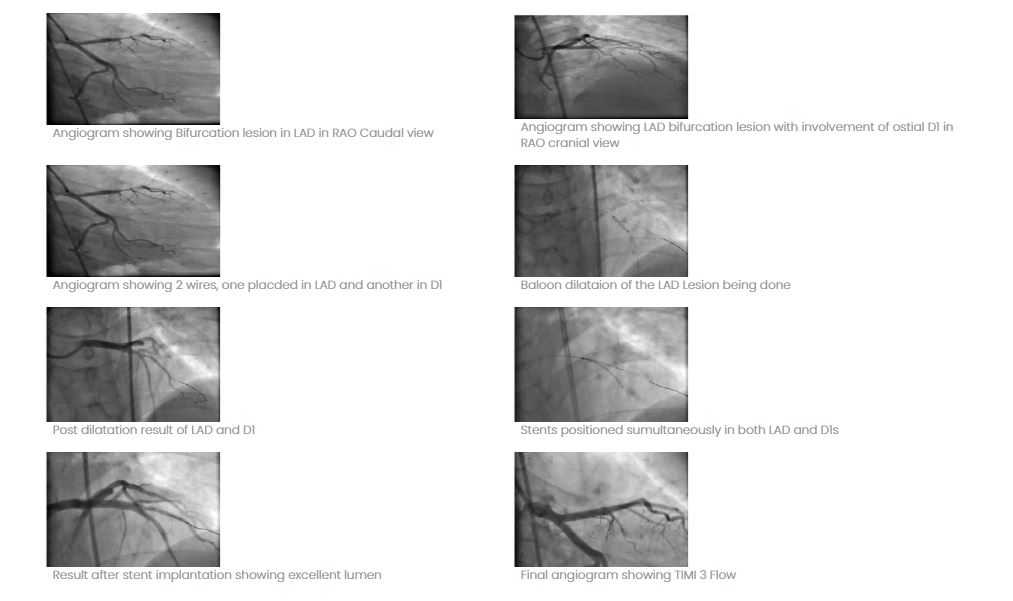
At Indo US Hospital, we have recently performed a case of complex angioplasty by a relatively new technique called “SKS” (Simultaneous Kissing Stents). A 40 year man presented with unstable angina and angiogram showed a critical lesion of LAD (left anterior descending Artery) involving the bifurcation of LAD and large diagonal. After dilating both the vessels, 2 stents were simultaneously placed and implanted with excellent result. This technique is called “SKS” technique. This technique is used less often but if properly done gives excellent long term results. We have done it in 8 cases in the last 6 months and all of them are doing well.
- Case Study 1
- Case Study 2
- Case Study 3
- Case Study 4
- Case Study 5
- Case Study 6
- Case Study 7
- Case Study 8
Interesting Case done at Indo US Super speciality Hospital, Ameerpet, Hyderabad
At Indo US Hospital, we have recently performed a case of complex angioplasty by a relatively new technique called “SKS” (Simultaneous Kissing Stents). A 40 year man presented with unstable angina and angiogram showed a critical lesion of LAD (left anterior descending Artery) involving the bifurcation of LAD and large diagonal. After dilating both the vessels, 2 stents were simultaneously placed and implanted with excellent result. This technique is called “SKS” technique. This technique is used less often but if properly done gives excellent long term results. We have done it in 8 cases in the last 6 months and all of them are doing well.